Predicting Poor Voiding Pattern after HoLEP using Maximum Flow Rate (Q-max) as an Objective Outcome
Abdulmalik Addar1, Adel Arezki1, Abdullah Alzahrani1, Hend Alshamsi1, Abdullah Alahmari1, Ahmed Ibrahim1, Abdulghani Khogeer1, Mélanie Aubé-peterkin1, Serge Carrier1, Fadl Hamouche1.
1McGill University, Division of Urology ,
Introduction:
Benign prostate enlargement (BPE) management has evolved significantly with the advances in medical technology and surgical technique. Holmium laser enucleation of the prostate (HoLEP) has emerged and is considered the size-independent gold standard for surgical management of BPE.1 Unfortunately, not all patients have excellent voiding after relieve of obstruction caused by BPE. This study aims to identify preoperative patient characteristics that predict poor voiding patterns after HoLEP using post-operative maximum flow rate (Q-max) as an objective measurement.
Methods:
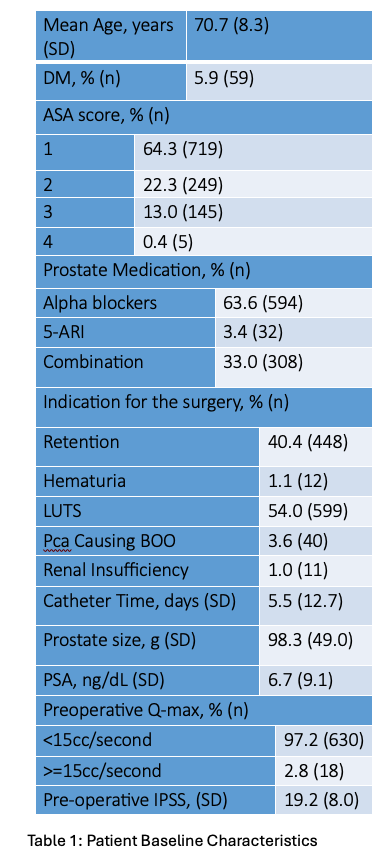
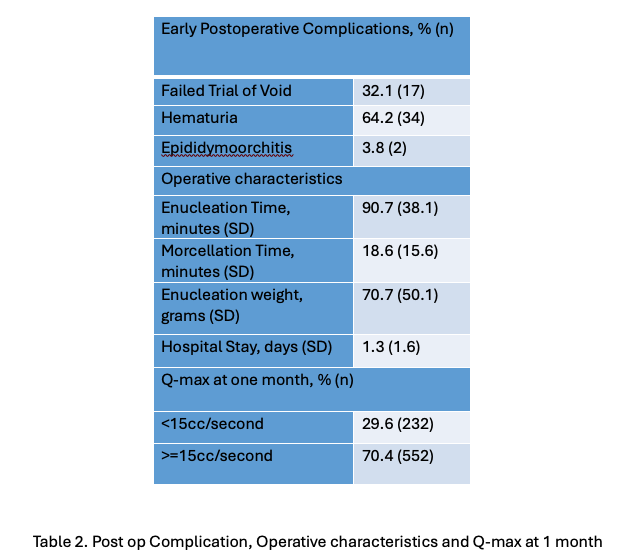
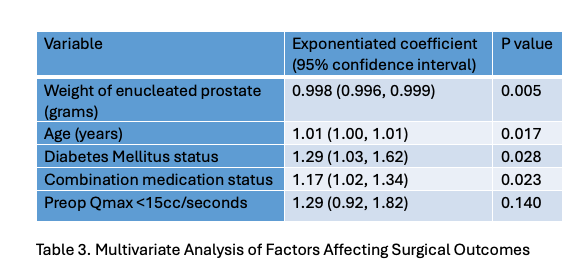
A Retrospective chart review of all patients undergoing HoLEP procedures at our institution between January 2006 and December 2022 was performed. Patient demographics, preoperative PSA, IPSS score, Qmax and catheter time were collected. Postoperative catheter time, trial of void results, IPSS score, and q-max were obtained. Predictive factors of poor emptying, defined as Qmax <15 ml/sec, were identified using logistic regression models.
Results:
A Total of 1121 Holep procedures were analyzed. The mean age was 70.78.3, the mean prostate volume was 98.349, and the mean hospital stay was 1.3 days ±1.6. low q-max was found in 232 (29.6%) at 1-month follow-up. Diabetes mellitus (DM), weight of enucleated prostate, being on combination medication for BPE and low preoperative q-max were identified as independent risk factors for low q-max. They had an OR of 1.29, 0.998,1.16 and 1.29, respectively (p-value< 0.005). Age had an OR of 0.0066 p=0.057, which may suggest it is a dependent risk factor for low q-max.
Conclusion:
Diabetes mellitus, a larger volume of enucleated tissue, being on combination BPE therapy, and low preoperative q-max are risk factors for low q-max post-HoLEP. Understanding these factors can help improve patient counselling and follow-up.
Présentations par / Lectures by Abdulmalik Addar
| Quand | Session | Titre | Salle |
|---|---|---|---|
|
ven.-08 08:15 - 08:45 |
SESSION I | PREDICTING POOR VOIDING PATTERN AFTER HOLEP USING MAXIMUM FLOW RATE (Q-MAX) AS AN OBJECTIVE OUTCOME | Salle de bal |